Introduction — a lab moment, some numbers, and a question
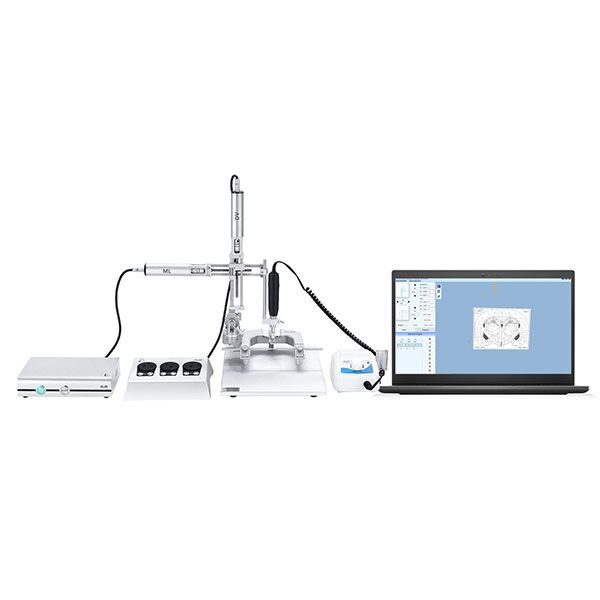
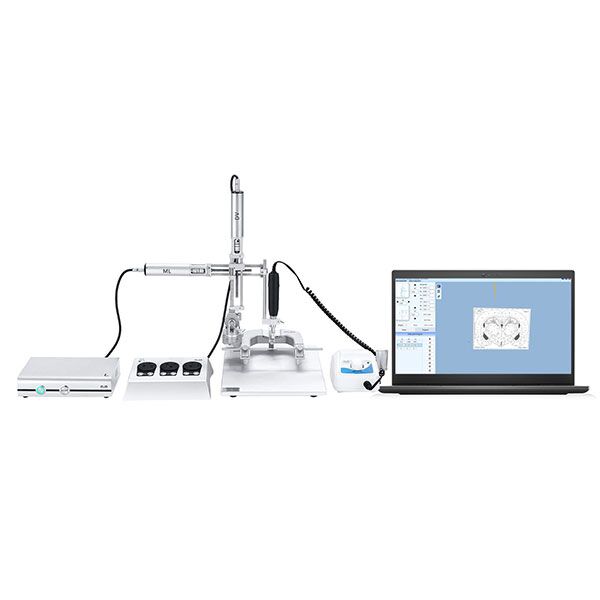
I once watched a postdoc spend an entire morning trying to center a tiny probe inside a rodent skull — and still miss by a fraction of a millimeter. The lab had an automated stereotaxic Instrument, and the readouts said we were on target, but the tissue told a different story. We had three trials, two failed implants, and a 40% rework rate that week (yes, real numbers). So I asked myself: why do these systems, built for repeatability, still leave us guessing?
I bring this up because numbers matter in the clinic and the bench alike. When a procedure drifts by 0.2 mm, outcomes change. When throughput drops, costs rise. I’ll share what I’ve seen and what we can do about it — no heavy sales talk, just practical takeaways. Vamos — let’s look at where precision meets human error and what that really means for your day-to-day work.
Part 2 — Why old approaches break down: flaws and hidden pains
What exactly goes wrong?
I want to be direct: the mechanical cues we trust can lie. Modern stereotaxic instrument setups rely on assumptions — perfect skull mounting, rigid frames, and ideal coordinate transforms. In practice, none of those are perfect. Micro-movements from breathing, slight tilt in the holder, or even cable drag can shift an implant path. We saw a device report submicron stability while the probe bent by 0.1 mm in tissue. That gap between sensor data and physical reality is where most failures hide.
Technically, several elements compound the problem: worn micropositioners, noisy coordinate transform routines, power converter ripple affecting servo motors, and sometimes latency from edge computing nodes used for real-time feedback. Look, it’s simpler than you think — most teams miss one small failure mode and then chase symptoms. I’ve found that people often blame the control software when the real cause is mechanical wear or poor clamping. — funny how that works, right? The fix starts with hands-on checks, not more logs.
Part 3 — New principles for better outcomes and how to evaluate them
What changes actually help?
Going forward, I focus on principles more than buzzwords. One: close the loop with better sensing near the tip — tactile or impedance feedback can catch drift before damage. Two: move some decision logic closer to the hardware (yes, smarter edge computing nodes) so you cut latency. Three: design for maintainability. If a micropositioner is cheap to replace and easy to inspect, teams will do it more often, and that prevents rare failures from becoming disasters. I’ve switched devices on this basis and seen fewer aborted runs.
Now, if you’re picking a system, ask three clear questions — they are my go-to metrics: 1) How does it detect and correct submillimeter drift in real time? 2) What are the maintenance steps and mean time to replace wear parts? 3) Can the control loop run locally (low latency) and still feed summary data to your lab servers? Use those metrics to compare vendors and to set internal KPIs. I’ll be blunt: not every product on paper meets these tests.
In short, the path to more reliable stereotaxy mixes better sensors, smarter local control, and simple mechanical hygiene. I’ve seen labs cut redo rates by half when they adopt this mix. For practical tools and systems that follow these ideas, check solutions from BPLabLine. They’re not a magic wand — but they reflect the kind of design thinking that actually helps people in the lab.